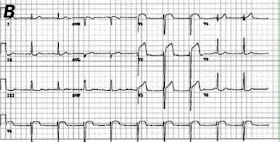
The ECG:
 |
| The computer interpretation used caps lock, had a lot of "***." |
Cardiology was skeptical, but had him in the cath lab 30 minutes later. My resident put 50 cents down on a LAD occlusion, while I bet him a cup of (free) coffee that this was a classic first diagonal , or high lateral, STEMI. The two cardiology fellows agreed that we were both mistaken, and that they were certain to find a blocked circumflex. While the patient was in the lab the troponin came back as significantly elevated.
A few hours later, the cards fellow calls me back with the cath results.
Survey says!
 |
| No offense to Steve Harvey, but I'm a Dawson kinda guy. |
Nada. Clean cath. "No significant fixed obstructive disease."
Interestingly, however, both ventriculography and an echo revealed hypokinesis of the high anterolateral wall, corresponding to the anatomy suggested by the ECG. He was given a diagnosis of focal myocarditis.
Focal Myocarditis
This isn't very common, but we can't say how uncommon. It is still uncommon enough to be worthy of case reports, at least in Texas. We know that about 3% of MIs have clean coronary arteries by angiography, but a number of those people have spasm or spontaneous reperfusion. The percentage may even be smaller with STEMI patterns, but we don't know.
The only way in the past to definitively diagnose myocarditis was through endomyocardial biopsy, which has a good number of shortcomings, in terms both of sensitivity, and of complications.
 |
| What could go wrong with this? |
 |
| Uh, yeah, I see it too... |
Now, I understand that the myocarditis can generate ST elevation, likely in the same manner that pericarditis does. I am really surprised, however, that our patient had such distinctive and appropriate reciprocal changes. Nonetheless, an ECG from a case report of myocarditis also shows reciprocal changes:
Turning to Stephan Smith's ECG Blog for some wisdom, I found this observation in "Is it MI or pericarditis?" (There's a lot of overlap between pericarditis and myocarditis, and many people link them on a spectrum; e.g myopericarditis.):
Pericarditis should never be assumed when there is even a hint of reciprocal ST depression. Only localized pericarditis (most pericarditis is "diffuse" inflammation of the entire pericardium) ever has reciprocal ST depression, and localized pericarditis is very rare. I suspect that many cases of "localized pericarditis" are really STEMI that went undiagnosed.
A great review article by Punja 2010 gives a few examples of ST elevation in myocarditis, but neither example shows reciprocal changes.
 |
| Nasty STE in myocarditis, but no ST depression |
The Bottom Line
So, the next time you bring in that "for sure" STEMI, keep in mind there's a (3%*78%=) 2% chance it's myocarditis. Or higher. Or lower.
Fascinating stuff. 78% is a big enough number to get anyone's attention. But now what I want to know is: what's the prevalence of myocarditis in asymptomatic patients from a similar cohort? And how many ACTUAL STEMIs (i.e. occlusion found) also have myocarditis? I mean, what we really want is to come up with some likelihood ratios, right?
ReplyDelete(I would have voted circumflex, by the way... LAD is a real stretch I think.)
ReplyDeleteBrandon brought this highly interesting post of your to my attention. I would make several points:
ReplyDeletei) Rather than the first diagonal branch of the LAD (which is likely when in the setting of acute ST elevation anterior MI you also have ST elevation in I,aVL) - IF this 35 yo male had had an MI - I would guess the circumflex as the culprit artery.
ii) GREAT POINT that you make about acute myocarditis (diffuse or focal) being the etiology of ST elevation in some unknown number of acute chest pain with ST elevation patients. This entity is NOT commonly thought of - and as you point out, it should be part of the differential.
iii) THANK YOU for the link to the Sarda et al 2001 JACC article on 'Myocarditis in Patients with Clinical Presentation of MI and Normal Cath' - it is excellent and highly insightful!
iv) Nice that invasive biopsy seems no longer to be needed to make presumptive diagnosis.
v) Initial management of this 35 yo man with chest pain and focal ST elevation (esp. given the reciprocal changes that are present) - is still be the same - immediate cath for suspected STEMI and possible PCI pending results. So - the approach on the "front lines" is the same ....
vi) Great questions asked by you & Brandon - about how common acute myocarditis really occurs (and how often it occurs without us knowing it ... ).
vii) That 3% figure that seems to often be quoted as the frequency of "acute MI with normal coronary arteries" is suspect - at least from what is reported in this Sarda paper that you frequently refer to in your post. Sarda cites 2 references for this statistic (Refs #15 & 16 in their paper). Ref #15 is by Betruiu et al - it is from 1981 based on a relatively small group of 259 patients, of which 8 had normal coronary arteries. Of note - is that these 8/259 patients were relatively YOUNG (none over 50; and 5 of the 8 were under 35 !!!).
viii) I could NOT get specifics of the other Ref #16 - by Lindsay et al (no abstract available and I don't have access to the actual paper) - but this Lindsay paper was written in 1984. So to me - we DON'T KNOW if this 3% figure is accurate - because it was based on caths done over 25 years ago ..... AND - there seems to be a definite trend for MOST of those patients who present with acute chest pain and ST elevation but normal cath to be YOUNGER. So my guess (no way of knowing unless anyone can find any good literature) is that it is substantially LESS than 3% of older patients presenting with acute ST elevation and acute chest pain who will have myocarditis rather than STEMI as their etiology ....
ix) Over the years in primary care - I'd see occasional patients who on presentation had severe cardiomyopathy without predisposing alcohol, smoking, cocaine,etc - which I presumed may have been the result of "silent myocarditis" - though of course that was never proven ....
BOTTOM LINE - Great post that brings to our attention the often overlooked entity of acute myocarditis that can at some unknown frequency be the cause of acute ST elevation with normal coronary arteries. This seems to be quite rare - and is especially (as best I can surmise) rare in patients over 50. It is the younger patient (in the 30-50 range) with new chest pain who might be more inclined to get acute myocarditis. As you point out - you CAN see reciprocal depression with acute myocarditis (unlike 99% of acute pericarditis cases in which there is no ST depression) - so the initial approach will be the same (Call Cards for acute cath) - but IMPORTANT for us to be aware of the entity of acute myocarditis that can on rare occasions occur.
THANK YOU for presenting this! - : ) Ken Grauer, MD (ekgpress@mac.com)
Found another number for rate of "clean caths," from the Gusto IIb investigators (http://www.nejm.org/doi/full/10.1056/NEJM199907223410402#t=abstract) - up to 10% of patients with MI.
DeleteNow, I can't believe that 78% of 10% of MI is actually myocarditis, but perhaps, as you say, this is more the case in the younger patient.
Hi Brooks. Thanks for your comment. I must admit that I'm not seeing specifically where in the NEJM the 10% figure comes up (I perused the article, but admittedly did not go over every word...). Would be great if you could e-mail me specifics as to WHERE this 10% figure comes up and/or post them here on this site. Acute myocarditis is not nearly that common - I strongly suspect it is rare ... Sincerely- Ken Grauer, MD (ekgpress@mac.com)
ReplyDeleteI hope it's rare! Otherwise I've missed a good number of cases.
DeleteTable 2 in the article, I was looking at the # of patients with either STE- or non-STE-MI who had 0 (zero) diseased vessels. I suspect that someone out there can speak to this issue with more authority than myself, however!
Hi Brooks. I went back to the article and looked at Table 2 - which compares 'severity' of CAD (number of vessels involved) between men vs women. This Table 2 does show that up to ~10% of women who had MI in this GUSTO IIb trial had "no vessels involved" on cath. However - I could not find anywhere in the article WHEN this cath was done. Perhaps I missed this ... but there are other reasons why an infarct (defined in this 1999 study by elevated CK-MB, since troponins weren't being used at the time....) may have "no vessels involved" other than myocarditis. If cath was done a day or more after the onset of symptoms .... there may have been resolution of the clot. I also don't see in this article how "involved vessel on cath" was defined ... Perhaps these details are described in the earlier (1996) initial report of the GUSTO IIb investigators (I did not try to go back to that study ....).
ReplyDeleteA final point on this to note is mention that "the decision to cath was based on clinical factors" (only ~ 55% of the patients in this study were cathed) - so the % of patients with no vessels involved may have been subject to some bias depending on whether a patient was or was not cathed ...
That said - I think the BOTTOM LINES from your interesting initial post are still valid:
i) The diagnosis of acute myocarditis is OFTEN overlooked;
ii) Endomyocardial biopsy is no longer the standard for diagnosing myocarditis (suboptimally accurate; invasive) - so possible that newer noninvasive techniques will allow much easier diagnosis - enabling in the future a much better estimation as to how often this diagnosis really occurs;
iii) The presentation of acute myocarditis may be similar (if not identical) to that of ACS - with acute ECG changes of ST elevation and reciprocal ST depression (other changes of course could be seen);
iv) It may only be after the patient with new-onset chest pain and acute-looking ECG changes is found to have normal coronary arteries on cath that the diagnosis of acute myocarditis may be suspected;
v) There is a certain incidence of acute MI patients (confirmed by positive markers - troponins) who will have normal coronary arteries on cath. What this percentage is - is difficult to tell - as the literature varies, and it will depend on the age and sex of patients studied;
vi) Acute Myocarditis as a cause of new-onset chest pain with ECG abnormalities and positive markers but normal coronary arteries on acute cath may be more likely to occur in patients younger than 50. That said - acute myocarditis is probably rare - but DOES occur, so is important to be aware of. Hopefully in the future we'll have a much better "feel" for how often this really occurs.
THANKS again Brooks for bringing this entity to our attention.
I started on COPD Herbal treatment from Ultimate Health Home, the treatment worked incredibly for my lungs condition. I used the herbal treatment for almost 4 months, it reversed my COPD. My severe shortness of breath, dry cough, chest tightness gradually disappeared. Reach Ultimate Health Home via their website www.ultimatelifeclinic.com I can breath much better and It feels comfortable!
ReplyDelete
ReplyDeleteI was diagnosed with COPD four years ago and struggled with worsening symptoms despite using inhalers and medications. Last year, I tried a herbal treatment from NaturePath Herbal Clinic, and to my surprise, it made a huge difference. My breathing improved, the coughing eased, and my energy came back. I feel better than I have in years. If you're dealing with COPD, I highly recommend checking them out: www.naturepathherbalclinic.com.