Treating a kid with a fever seems like a no-brainer. It almost doesn’t seem to need any further justification - a fever is bad, and medicine to treat the fever is good. It’s right up there with mom and apple pie!
 |
| Did I say "no-brainer?" My bad! (source) |
It may appear like we're always taking drugs (e.g. atropine, furosemide) and devices (MAST pants, pediatric intubation) away from EMS, So, it seems pretty nifty to actually add a drug to the EMS formulary.
And why not? The medicines (Tylenol and ibuprofen) are relatively safe (even zombie moms are allowed to buy it for their babies), EMS can start the anti-fever therapy quickly, and we can prevent…. something.
And why not? The medicines (Tylenol and ibuprofen) are relatively safe (even zombie moms are allowed to buy it for their babies), EMS can start the anti-fever therapy quickly, and we can prevent…. something.
Wait a minute, what are we actually treating? And why is treating a fever so darn important that EMS should do it?
1. There is no agreement on when to "treat a fever."
Tylenol and ibuprofen are used to reduce fever, and to treat discomfort, and are near-universal therapies for kids and adults.
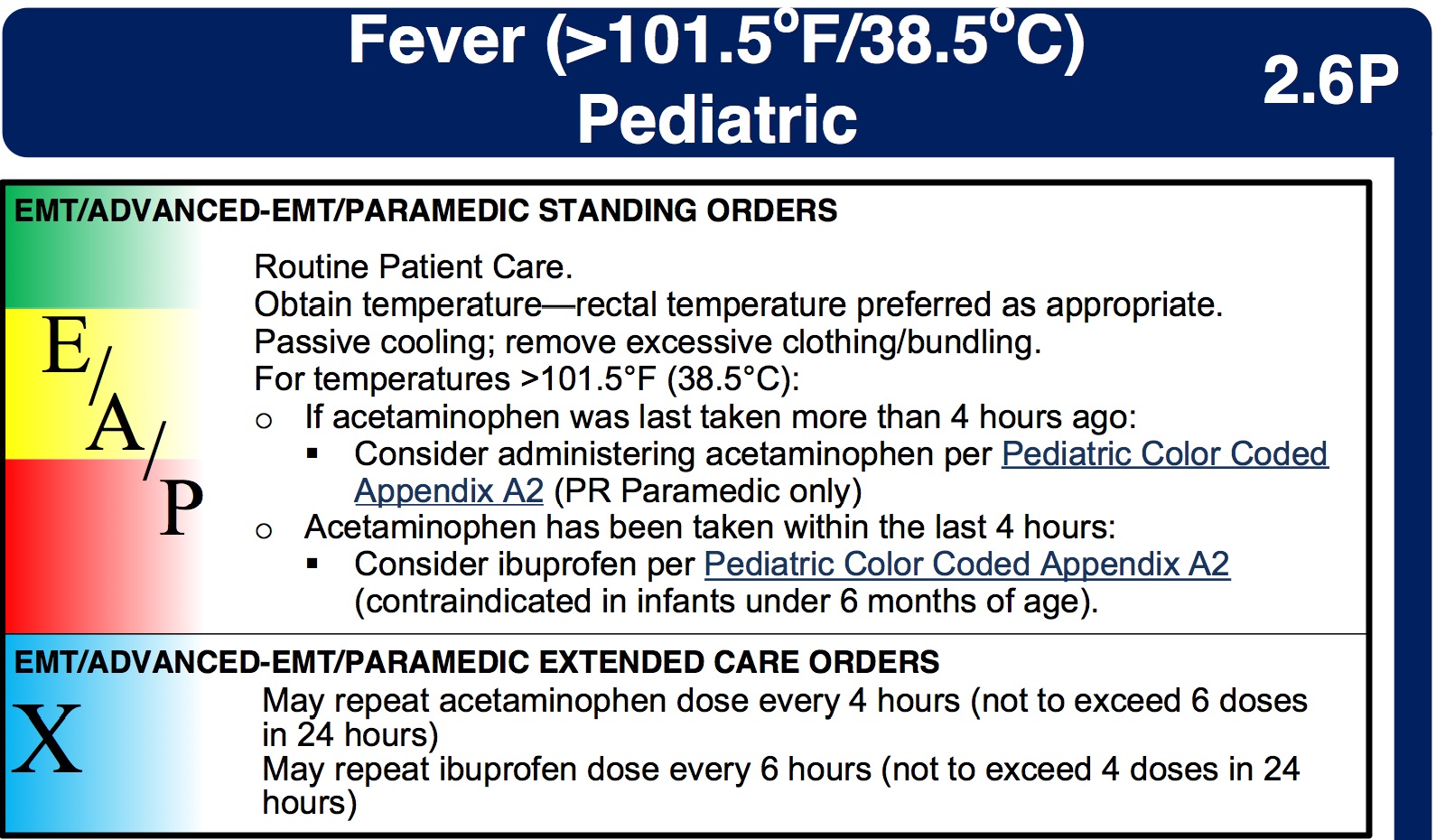
Treating mild discomfort is a great idea, since not all pain needs morphine. But protocols, in general, only mention a number (temperature) as a trigger for antipyretic use, and most protocols can’t even agree on which number that should be. You can find examples of fever "triggers" for antipyretic use at 100°, 100.2°, 100.4°, or even 101.5°.
For example, check out the New Hampshire state protocols:
For example, check out the New Hampshire state protocols:
It turns out there’s a good reason why there is no agreement on what temperature "needs" APAP - nobody knows!
And not only is there no evidence saying what temperature elevation needs antipyretic therapy...
2. Fever isn’t dangerous!
While having a fever is unpleasant, there is no evidence that it is harmful. In fact, most experts agree that damage can’t occur until the temperature has been over 106° for a while, which is almost unheard of for an infectious cause.
(Hyperthermia - as in heat stroke - is a entirely different matter, and brain damage can occur quickly, even below 106°. But no one talks about giving Tylenol to a kid that’s been locked up in a car during summer.)
The American Academy of Pediatrics makes it pretty clear
Yeah, we should treat pneumonia or meningitis with antibiotics (or heatstroke with ice), but there is no benefit to Tylenol besides feeling a little better.There is no evidence that reducing fever reduces morbidity or mortality from a febrile illness.
3. It won’t stop a febrile seizure, or keep it from happening again.
Yes, febrile seizures are often unsettling to parents, but they are essentially harmless. Per the experts:
As the AAP guideline on febrile seizures notes that (my emphasis):
There is a theoretical risk of a child dying during a simple febrile seizure as a result of documented injury, aspiration, or cardiac arrhythmia, but to the committee's knowledge, it has never been reported.But OK, they aren't, like, medically bad, sure. But why not quickly treat the fever in a kid who just seized, or who has a history of febrile seizures and just spiked a temp? Well, a number of studies have been done on the subject, and they all say the same thing - aggressive use of Tylenol or Advil does nothing to prevent the next febrile seizure. Phenobarbital or valium do prevent them, but they have significant side effects.
As the AAP guideline on febrile seizures notes that (my emphasis):
In situations in which parental anxiety associated with febrile seizures is severe, intermittent oral diazepam at the onset of febrile illness may be effective in preventing recurrence.
The paramedic’s job should be to reassure (when appropriate) the parents, and treat any mild discomfort associate with a fever. Wrestling a kid to give them Tylenol “to get their fever down” isn’t worth it, and likely doesn’t do much to help their mild discomfort.
I'm also not sure how much the wrestling helps treat the "severe parental anxiety!"
I'm also not sure how much the wrestling helps treat the "severe parental anxiety!"
4. In adults with septic shock and fever, antipyretics could increase mortality
A recent issue of Chest (a journal for pulmonary/critical-care physicians) featured a spirited debate on whether septic patients with a fever should be cooled.
The only point on which everyone agreed was that antipyretics like Tylenol or ibuprofen weren’t useful, and could in fact make the situation worse. As the "pro-cooling" team in the debate conceded,
“Little evidence-based support exists for use of antipyretic medications to improve fever-associated morbidity and/or mortality.”
5. It may promote “fever phobia” in parents and medical providers.
By carrying the drug, and promoting its early use, EMS may play a role in driving "fever phobia." This is the name for the belief that many parents (and far too many doctors and nurses!) have, that fevers are very dangerous. As the expert pediatricians at the AAP put it, too many doctors and nurses worry about fever causing seizures, brain damage, or death. They then pass on these irrational concerns to the public. As they put it:
It is argued that by creating undue concern over these presumed risks of fever, for which there is no clearly established relationship, physicians are promoting an exaggerated desire in parents to achieve normothermia by aggressively treating fever in their children.As a consequence, our medical offices, emergency departments, and EMS systems get many calls for a "kid with a fever," who doesn't otherwise look sick, wasting time and money, sometimes prompting unnecessary tests, and in general causing a whole bunch of bother.
The Bottom line
Giving Tylenol or Motrin, in accordance with your protocols, is fine. These are very safe drugs, and they do well at treating small aches and discomforts. But keep a realistic view of what you are using them for. And try to avoid spreading any medical myths!
In situations in which parental anxiety associated with febrile seizures is severe, intermittent oral diazepam at the onset of febrile illness may be effective in preventing recurrence.
ReplyDeleteShould that intermittent oral diazepam be given to the parent or to the child?
Parental diazepam may be effective in preventing recurrence of the parental anxiety.
Similarly, administering diazepam (I would love to have a Midazolam Mist device to spray anxious people) to doctors, nurses, medics, . . . should be effective at reducing fever phobia.
And try to avoid spreading any medical myths!
I will have to work on that. ;-)
.
You know, I wonder if the authors of the AAP statement had a little fun, leaving the slightest hint of ambiguity in the wording?
DeleteEther would be another choice, but only for anxiety and anxiety-induced seizures.
DeleteThe Bugs Bunny protocol.
https://www.youtube.com/watch?v=DS0kFhrd4DI
However, ambiguity can probably be cured with ribavarin. O_o
http://www.sciencebasedmedicine.org/ambiguity/
http://www.pusware.com/quackcast/quackcast67.mp3
.
I was also wondering if the oral diazepam was being recommended for the severely anxious parent.
DeleteI'll bet we could garner as much fever relief from giving the child a cowbell as we could with antipyretics.
ReplyDeleteBut we need a specific dose.
DeleteMore is not an acceptable dose.
The noise monitors would be set off regularly.
Cowbell toxicity can be serious.
People could begin to act like Christopher Walken. I don't want to wear a wrist watch in a world where people act like Christopher Walken.
.
I didn't intend to toss the (febrile) baby out with the (tepid) water! APAP and the NSAIDs are a cornerstone of pediatric emergency medicine. Heck, along with Popsicles, they account for 95% of our therapy.
DeleteHey, I have an idea... how about studying Tylenol, Popsicles, and cowbells as a bundled intervention?
Another area where paramedics feel a need to "do something" when doing nothing but taking the patient to the hospital would be better. Even better, as you allude, would be if parents wouldn't call 9-1-1 for "baby with fever", especially when all they want is a trip to the ED so they can get a script for pedi APAP so that they don't have to pay cash for it.
ReplyDeleteI'm dreaming about that last part, of course.
Certainly, if the choice is between "do nothing (but drive) for the child who has a fever but is breathing, drinking, and mentating just great," and "pry open the oh-so-vigorous kid's jaws to squirt in the elixir of antipyresis," I would vote for the more passive approach!
DeleteNot to cast aspersions on your side of the equation doctor, but there are some doctors who would be better medical directors if they would impress on the paramedics in their system(s) that often doing less is better for the patient.
DeleteI believe that this discussion goes hand-in-hand with the over prescription of antibiotics. Healthcare providers have to deal with both external (parents) and internal (“I got into this to help people”) pressures "do something!” which can be pretty strong when you have an actual sick child in front of you. That’s why, even though I often don’t get very far with it, I try to promote the idea that assessing, assuring and advice IS doing something and that very often giving meds may help with a complaint, but not actually fix the problem. Laypeople can somewhat be forgiven for not knowing the difference between a complaint and the actual underlying problem, but as healthcare providers we should know better and educate our patients and / or their parents as best we can.
ReplyDelete" I try to promote the idea that assessing, assuring and advice IS doing something..."
DeleteIt turns out that there is great research that backs you up on that. One study looked at what both the parents and the physicians were expecting during a sick-child visit to the ED, and what actually affected satisfaction.
Turns out, the parents' satisfaction was much more closely tied up with how well the doctor explain the diagnosis, the attention they paid to the child, and the level of concern they had for the child's comfort. Giving a prescription for abx, OTOH, didn't affect parental satisfaction.
Still, on a different tack, do you feel that with the current limitations on EMS alternative transport destinations (other than ED) that the in-home administration of tylenol and contact with the primary pediatrician may be of benefit if it defers the unnecessary transport to the ED that the parents may demand if they feel the child is still sick?
ReplyDeleteTough to feel confident deferring transport of a sick kid, and the liability of a bad outcome, while very rare, would be significant.
DeleteOn the other hand, it seems that some EMS agencies frequently get called solely to provide Tylenol, with no desire for transport. If that's the case in your region, this might be a popular protocol!
As you note the liability for a bad outcome is significant. While an ED visit might not be optimal, at 0300 in the morning, what is the alternative? Paramedics are notoriously bad at deciding who does and doesn't need to go to the hospital. Phone triage systems that some HMOs and primary care clinics aren't any better.
DeleteWe all laugh at the "Baby with a fever" calls, but one of my last cardiac arrest calls was for a seven year old whose aunt was assured by the nice lady on the phone at the clinic that it was just a fever and Tylenol and fluids would take care of it.
Rommie, just how do you propose to get in touch with the primary pediatrician and get an answer in a timely fashion? Especially during off hours when the call is going to go to an answering service.
This comment has been removed by a blog administrator.
ReplyDeletedoes anyone have or seen a protocol using torodol as an antipyretic. I have found studies saying it as good as Tylenol, but nothing saying it is or can be used.
ReplyDeleteI had only read about such a fantastic post, love to read this information on see this and now I see it here on blog and I can't contain myself. It is such an amazing and perfect place for a person to start a new life
ReplyDeleteThanks for sharing such beautiful information with us. I hope you will share some more information about fever. Please keep sharing.
ReplyDeleteHealth Is A Life