The mother states the child has had 1 hour of progressive respiratory distress after being stung by a bee. The initial vitals are BP 76/40, P 120, R 45, and SpO 91% on room air. The patient is sitting upright, speaking in short sentences, and has audible wheezing. The physical exam reveals hives over the chest and arms. If you don't act in 2 minutes, your patient will decompensate. What do you do?
(By the way, this is a HIPAA-compliant picture of your patient:)

Yup, it’s a replicant, and just like Roy Batty, he was programmed to die in this EMS simulation study performed in Michigan.
Unlike Roy Batty, however, this replicant will live if he is given epinephrine in time!
 |
| "I've seen things you people wouldn't believe... And I need some epi!" |
The authors used a high-fidelity simulation manikin, in a well-equipped simulation center, as well as the scenario described above. They allowed the EMS crews to use their own medication and equipment, but they all had to follow the state EMS protocol for pediatric anaphylaxis.
 |
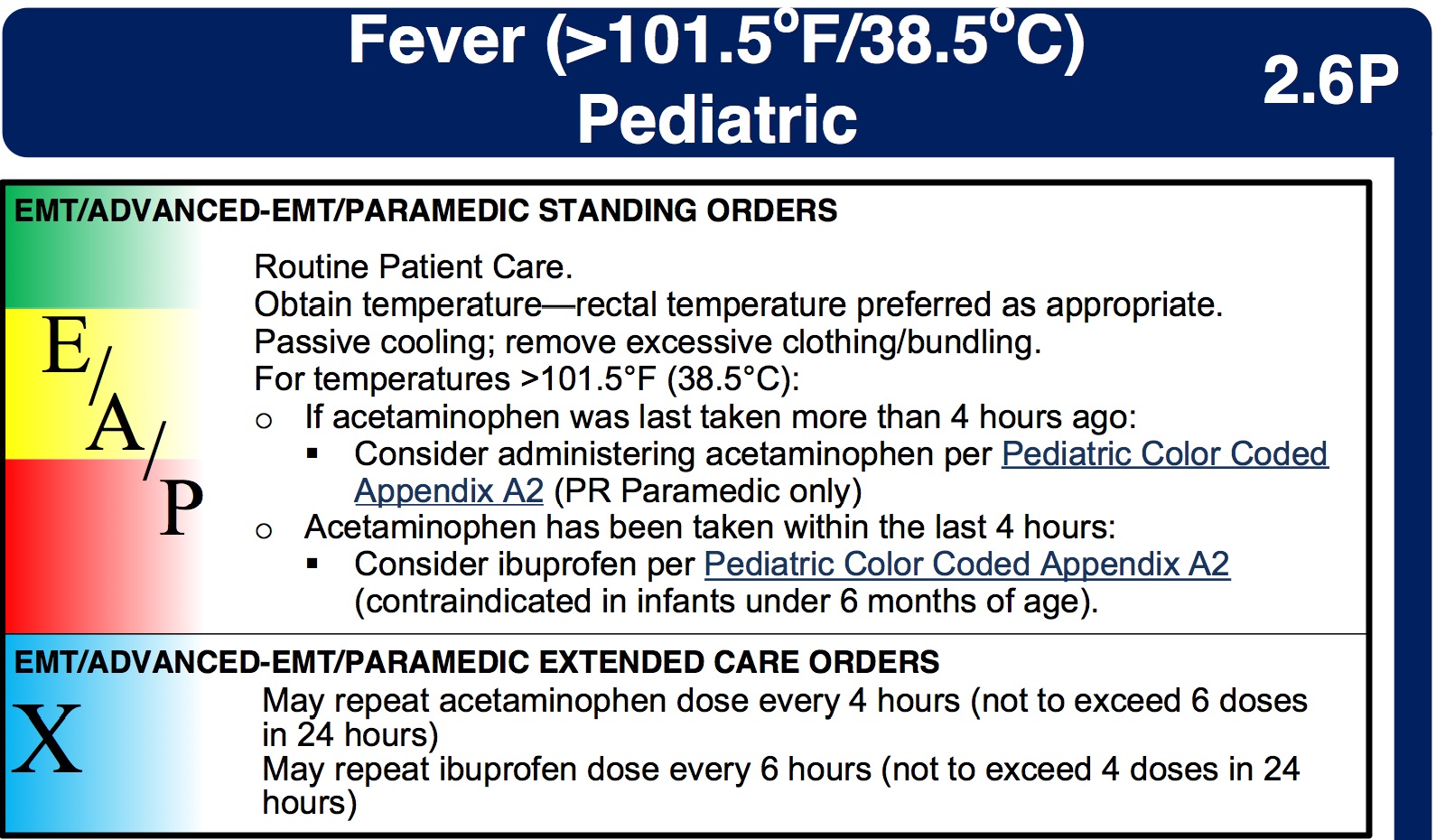
| Michigan EMS protocols |
If the crews gave the right medications and interventions, the kid got better. If not....
So what happened?
Before I answer that, let me point out that the EMTs and medics volunteered for this study. This suggests that these folks were motivated enough to participate in research, aware they were going to observed, and fairly confidant in their knowledge and skills. In other words, probably some good, smart people.
So, it's all the more distressing what the study found.
1. Three out of 62 crews (5%) did not give epi
For true anaphylaxis, epinephrine is the required treatment, with essentially no contraindications.
2. Epi was often given by the wrong route.
The protocol spelled out that epinephrine should be given IM, in line with several national and international guidelines. Despite this, only 37 out of 59 (63%) crews gave epinephrine IM. The authors were generous, and allowed SQ as an acceptable route, but this is an outdated practice.
3. An epi dose of > 1 mg was given by 20% of crews.
‘Nuff said about that...
4. Epi was given intravenously by 15% of crews
Although IV epi is listed in the protocol, even "low" doses of IV bolus epi can cause badness. With that in mind, the protocol allowed for IV epinephrine only “in cases of profound anaphylactic shock (near cardiac arrest).”
Because the patient was initially sitting upright, speaking, and perfusing, IV epi was considered a major error.
5. Less than half of the crews gave epi by the right dose and route.
As shown in this table:

So why did this happen?
It's hard to manage a rare medical event, using a drug that is available in multiple concentrations, and can be given by multiple routes, but must be dosed accurately by weight.
And as I said before, these were engaged and motivated EMS providers. Furthermore, the errors that they committed have been demonstrated to occur in a number of prior studies and case reports, involving a wide range of medical personnel.
In other words, you can’t respond to this study by saying “Well, our guys would never screw up like this!” Or by saying “We’ve been doing it this way for years without a problem.” This study should force all of us to reevaluate how we teach, protocolize, and practice treatment of anaphylaxis.
If you have the patience, download the author’s summary (the picture below) of the types of errors that were committed, and the rationale of the medics who committed them. Very informative!