 |
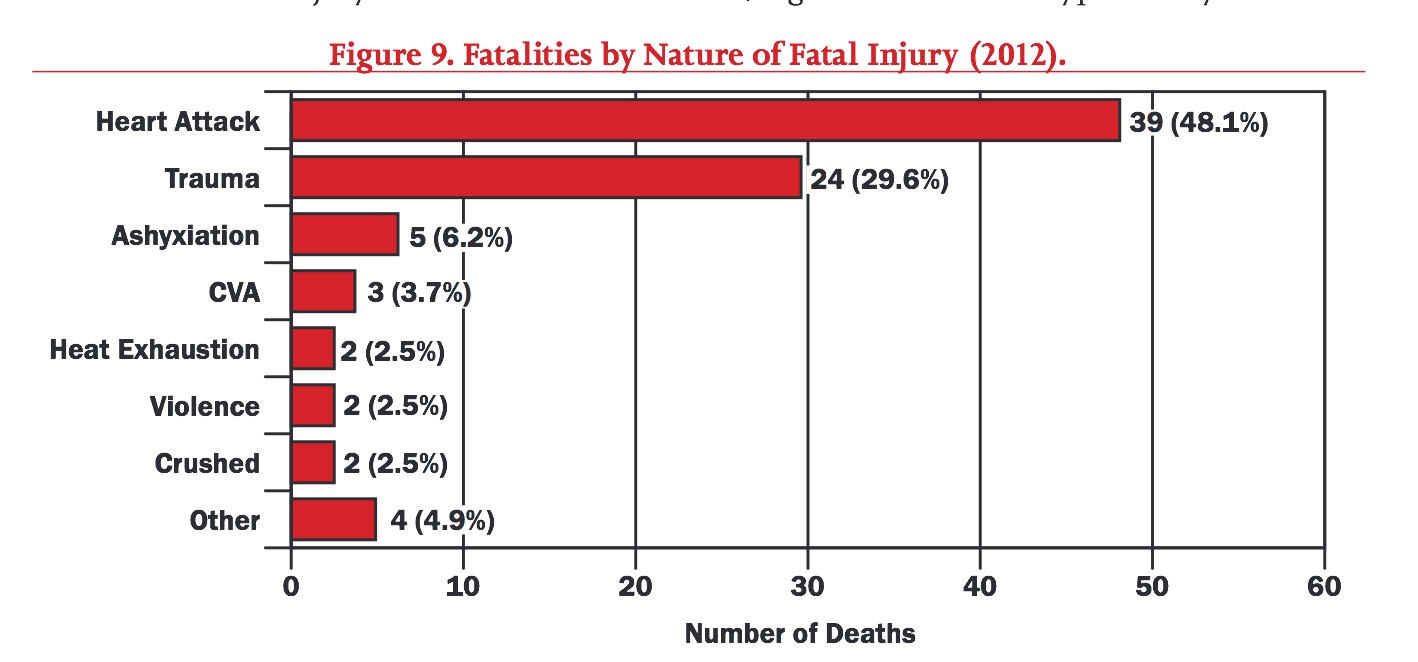
| From a 2012 FEMA report |
The chart above comes from the 2012 USFA report of firefighter fatalities, and it’s shocking. Over half the fatalities in that year had nothing to do with burns, entrapment, falls from ladders, or other traumatic dangers. Instead, MI and stroke, in general, were the biggest danger firefighters faced.
Now, this is partly a function of age, but 15% of the deaths from MI were in firefighters younger than 45 years old. A recent study focused on this group, and found some surprising results.
The Study
The authors of Sudden Cardiac Death Among Firefighters ≤45 Years of Age in the United States wanted to take a closer look at these younger firefighters who died of cardiac causes, and see if there were any risk factors that could explain those deaths.
To do this, they used the database maintained by NIOSH (http://www.cdc.gov/niosh/fire/) to find all cases of firefighters < 45 years of age who had a sudden cardiac death. They looked at the period from 1996 to 2012, and examined autopsies and other reports.
The authors of Sudden Cardiac Death Among Firefighters ≤45 Years of Age in the United States wanted to take a closer look at these younger firefighters who died of cardiac causes, and see if there were any risk factors that could explain those deaths.
To do this, they used the database maintained by NIOSH (http://www.cdc.gov/niosh/fire/) to find all cases of firefighters < 45 years of age who had a sudden cardiac death. They looked at the period from 1996 to 2012, and examined autopsies and other reports.
They then selected a bunch of age-matched, healthy, “occupationally active” control firefighters to compare them to. Additionally, they looked at noncardiac traumatic fatalities (deaths due to blunt trauma, burns, or asphyxiation) to serve as a second comparison group.
1. The FFs with sudden cardiac death
They found 87 FFs under the age of 45 who had a sudden cardiac death during that time.

- Almost all were men.
- Over 1/4 of them smoked
- (Only 18% of Americans smoke).
- Almost 2/3 (63%) of them had a BMI ≥ 30.
- (Versus about 36% of American males)
- Over 1/4 of them had a BMI over 35.
- Over 1/2 had evidence of both cardiac disease and cardiomegaly.
- (Only 40% of men age 40-59 have CAD, HTN, CVA, or CHF)
At first glance, it looks like these firefighters had much worse health than the general public. But maybe this is due to the unique stresses of the job. For example, disruption of normal sleep patterns could encourage sleep apnea, leading to hypertension and obesity.
So in order to clarify the issue, they compared the FFs who had sudden cardiac death with the people most like them - other firefighters!
2. Compared with occupationally active FFs
When they compared these FFs to the “occupationally active" FFs, however, they found concerning results, suggesting that the FFs who had cardiac arrests were indeed unhealthier than their own peers.
So in order to clarify the issue, they compared the FFs who had sudden cardiac death with the people most like them - other firefighters!
2. Compared with occupationally active FFs
When they compared these FFs to the “occupationally active" FFs, however, they found concerning results, suggesting that the FFs who had cardiac arrests were indeed unhealthier than their own peers.

Obesity, smoking, and hypertension were significant predictors of cardiac death while at work. Not unexpectedly, a history of cardiac problems was a huge risk factor as well.
3. Compared with FFs who had a traumatic death
When they then compared the FFs who died from sudden cardiac death to those that had a traumatic death, they found significant difference in both age, and in the size of their hearts. FFs who suffered a cardiac death had higher rates of cardiomegaly, or enlarged hearts, suggesting that they had had longstanding problems with hypertension or obesity (or both).

So what do we do with these results?
First off, prevention (i.e. lifestyle) trumps everything. Quitting smoking, keeping a healthy weight, and maintaining a vigorous exercise routine, amongst other things, may have gone a long way towards preventing many of these deaths. Although firefighting presents many unique challenges to staying healthy (e.g. schedules that disrupt sleep patterns, exposure to heat stress), the comparisons to healthy FFs, as well as those who died from trauma, show that smoking and hypertension play a huge role in raising the risk of cardiac death.
First off, prevention (i.e. lifestyle) trumps everything. Quitting smoking, keeping a healthy weight, and maintaining a vigorous exercise routine, amongst other things, may have gone a long way towards preventing many of these deaths. Although firefighting presents many unique challenges to staying healthy (e.g. schedules that disrupt sleep patterns, exposure to heat stress), the comparisons to healthy FFs, as well as those who died from trauma, show that smoking and hypertension play a huge role in raising the risk of cardiac death.
Second, we need to prepare for cardiac arrest in firefighters. The unique nature of the fireground, as well as the obstacles that the clothing and equipment present, mean that departments need to practice their response to a "fallen" firefighter, aiming to start CPR and assess for a shockable rhythm as soon as possible. This requires special procedures, teamwork and practice. Watch these guys from Hilton Head FD run through a drill.
Be safe, and take care of your heart!
Be safe, and take care of your heart!





















